If you’ve ever found yourself agonizing over whether your 8-month-old finished two tablespoons of peas or just one, you’re not alone. The question, “How much should my baby eat?” is one of the most common, and anxiety-inducing, queries in early parenthood. We live in a culture obsessed with metrics and quotas, but feeding an infant requires a different mindset—one of trust and observation.
This guide will provide you with the general baby portion sizes by age you’re looking for, grounded in recommendations from the American Academy of Pediatrics (AAP) and the World Health Organization (WHO). But more importantly, it will equip you with the foundational principle that overrides any chart: responsive feeding.
Your baby is the ultimate authority on their hunger and fullness. Our job is not to count calories, but to provide nutritious options at appropriate times, read their signals, and trust their innate ability to regulate intake. This approach, supported by leading health authorities, fosters a healthy relationship with food that can last a lifetime, reducing struggles and power dynamics at the table before they even begin.
We’ll move through the first year and into toddlerhood, translating developmental stages into practical feeding rhythms, offering visual portion guides, and debunking the myth of the “clean plate.” Let’s shift the focus from volume to variety, and from control to connection.
Chapter 1: The Foundational Principle – What is Responsive Feeding?
Before we discuss a single teaspoon, we must understand the core philosophy endorsed by the WHO, UNICEF, and the AAP.
Responsive feeding is a reciprocal process. It means:
- You provide safe, nutritious food at developmentally appropriate times.
- Your baby gives clear cues about hunger, enjoyment, and fullness.
- You observe, interpret, and respond to those cues promptly and supportively.
This is a dialogue, not a monologue. It applies to breastfeeding (feeding on cue, not on a rigid schedule) and solid foods alike.
Recognizing Hunger Cues (The “Green Light”)
- Early: Smacking lips, sucking on hands, turning head toward breast/bottle (rooting).
- Mid: Becoming more physically active, trying to position themselves for feeding.
- Late: Fussing or crying. It’s best to respond during early cues for a calmer feed.
Recognizing Fullness Cues (The “Red Light”)
- Early: Slowing pace, becoming distracted, playing with the nipple or spoon.
- Mid: Closing mouth tightly, turning head away, pushing food away.
- Late: Spitting out food, crying, arching back.
The Golden Rule: Respect the “no.” Forcing a baby to finish a portion after they signal fullness teaches them to override their internal satiety meter, which is linked to later obesity risk. The CDC emphasizes that trusting these cues is crucial for healthy growth.
Chapter 2: The First 6 Months – Liquid Nutrition Only
Portion Guideline: On-demand, cue-based feeding. There are no set ounces or milliliters that apply to every baby every day.
Breastfed Babies:
- Frequency: 8-12 times in 24 hours in the early weeks, gradually spacing out.
- Portion: Let your baby nurse actively until they release the breast, appear content, and show fullness cues. Offer the second breast. They will take what they need. Weight gain and wet diapers are the best indicators of sufficient intake, not stopwatch timing.
Formula-Fed Babies:
- General Averages (NOT mandates):
- Newborn: 1-2 oz per feed, every 2-3 hours.
- 1 Month: 3-4 oz per feed, every 3-4 hours.
- 4 Months: 4-6 oz per feed, 4-6 times a day.
- Crucial Practice: Practice pace-feeding (holding bottle horizontally, allowing pauses) to let baby control the flow and signal fullness. Never prop a bottle.
The Milestone: The AAP and WHO recommend exclusive breastfeeding/formula for about 6 months. The readiness for solid food introduction is signaled not by a date, but by developmental signs: sitting with minimal support, good head control, loss of tongue-thrust reflex, and showing interest in your food.
Chapter 3: 6 to 8 Months – The Explorer Stage
Goal: Introduce tastes and textures, not to replace milk. Think of solids as “complementary foods.” Breast milk or formula is still the primary source of nutrition.
Feeding Rhythm: 1-2 “meals” per day, offered about an hour after a milk feed so baby isn’t frantically hungry.
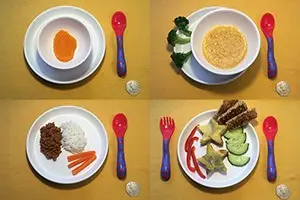
Visual Portion Guide (Per Meal):
- Cereal/Grains: 1-2 tablespoons of iron-fortified infant cereal mixed with breast milk/formula.
- Fruits/Vegetables: 1-2 tablespoons of puree.
- Protein: 1-2 tablespoons of pureed meat, beans, or yogurt.
- Total Meal Volume: Often just 2-4 tablespoons combined. A tablespoon is about the size of an ice cube.
Key Concepts:
- One Food at a Time: Introduce single-ingredient foods, waiting 3-5 days before adding another to monitor for allergies.
- Texture is Key: Start with smooth purees, quickly moving to thicker, mashed, and soft, lumpy textures to encourage oral motor development.
- Follow the Leader: If baby eagerly opens for more, offer another spoonful. If they turn away, stop. The first few tries might just be a taste. This is how much a 6 month old should eat—it’s highly variable.
Chapter 4: 8 to 12 Months – The Independent Eater Emerges
Goal: Solid foods become more substantial, contributing significantly to nutrition. Milk feeds begin to decrease slightly in volume.
Feeding Rhythm: 2-3 meals per day, plus 1-2 planned snacks. Offer solids first, then top off with breast milk or formula.
Visual Portion Guide (Per Meal):
Think in terms of tablespoons or small handfuls from each food group. A typical plate might include:
- Protein (1-4 tbsp): 2 tbsp shredded chicken, 1/4 scrambled egg, 2 tbsp crumbled ground beef.
- Fruits/Veggies (2-6 tbsp): 3 tbsp steamed broccoli florets, 1/4 mashed banana, 2 tbsp avocado slices.
- Grains (2-4 tbsp): 2 tbsp cooked pasta, 1/4 slice of toast strips, 3 tbsp cooked rice.
- Total Volume: Appetite varies wildly. A meal might be 1/4 to 1/2 cup of food total.
Key Concepts:
- Finger Foods: This is prime time for baby-led weaning or supplementing purees with soft, graspable finger foods (steamed pea-sized carrot pieces, soft fruit chunks, pasta shells).
- Self-Feeding: Expect and embrace mess. Let them hold a spoon, grab food, and explore. This builds motor skills and autonomy.
- Milk Intake: Breastfeeding may be 4-6 sessions per day. Formula intake typically caps at 24 oz max per 24 hours to ensure they have room for solid foods rich in iron and zinc.
Signs of Good Intake: Steady growth along their curve, a variety of foods eaten over a week (not every day), and increasing skill with chewing and swallowing.
Chapter 5: 12 to 24 Months – The Transition to Toddlerhood
Goal: Family meals. Your toddler now eats modified versions of what you eat. Milk becomes a beverage, not the main course.
Feeding Rhythm: 3 meals + 2-3 snacks per day, offered on a predictable schedule (e.g., meal every 2.5-3 hours).
Visual Portion Guide (Per Meal):
A useful rule of thumb from pediatric dietitians: One tablespoon of each food group per year of age. So, for a 1-year-old:
- Protein: 1 tbsp beans, 1 tbsp shredded meat, or 1/2 a hard-boiled egg.
- Fruit/Veggie: 1 tbsp cooked peas and 1 tbsp berries.
- Grains: 1 tbsp rice or 1/2 slice of bread.
- Dairy: 1 tbsp shredded cheese or 1/4 cup yogurt on the side.
- Total Volume: This often equals about 1/4 to 1/2 cup of each food on the plate. Their stomach is roughly the size of their fist.
Key Concepts:
- The Milk Shift: The AAP states whole cow’s milk can be introduced at 12 months. Limit to 16-24 oz per day to prevent iron-deficiency anemia and ensure appetite for solids.
- Appetite Slump: Growth slows dramatically. It is biologically normal for a toddler’s appetite to be erratic and small. They may eat a feast one day and barely anything the next.
- The Division of Responsibility: Ellyn Satter’s model is gospel here: The parent decides what, when, and where food is offered. The child decides whether and how much to eat. This relieves incredible pressure.
Chapter 6: Navigating Common Concerns – Beyond the Portion Chart
“My Baby Doesn’t Eat the Recommended Amounts!”
Charts are averages. Your baby is an individual. Consistent growth and energy are the true metrics. The Mayo Clinic advises that focusing on a baby’s overall development and demeanor is more important than comparing them to a generic portion size.
“He’s Such a Picky Eater!”
Especially around 12-24 months, neophobia (fear of new foods) is a normal developmental phase. Strategies:
- Repeat Exposure: It can take 10-15 exposures for acceptance. Serve a refused food without comment alongside a preferred food.
- No Short-Order Cooking: Offer at least one “safe” food at each meal, but don’t become a personal chef.
- Involve Them: Let them choose between two veggies at the store or help wash produce.
“Is My Baby Overeating or Undereating?”
- Overeating Cues: Rare in responsive feeding. Can happen if pressured or soothed exclusively with food. Stick to the schedule and trust fullness cues.
- Undereating Red Flags: Consult your pediatrician if you see a sustained drop off the growth curve, extreme fatigue, or fewer than 4-6 wet diapers a day.
The Role of Growth Charts
Your pediatrician plots your baby’s weight, length, and head circumference on WHO growth charts (based on breastfed infants). What matters is their own consistent curve, not their percentile. A baby at the 10th percentile following the 10th percentile curve is growing perfectly.

Conclusion: Cultivating Confidence, Not Control
The journey of how much should my baby eat is ultimately a lesson in letting go. We provide the scaffolding—the nutritious options, the regular rhythm, the calm environment—and then we must trust our children to climb it in their own way.
Ditch the measuring spoons as a gauge of success. Instead, measure success by:
- The joy of discovering a new flavor.
- The confidence of a baby feeding themselves.
- The peace of a meal without pressure.
- The steady, upward trend on their growth chart over months, not days.
Arm yourself with the general baby feeding schedule by age and portion visuals in this guide, but keep them in your back pocket. Keep your eyes on your child. Their cues are the most reliable guide you will ever have. When in doubt, your pediatrician is your partner in ensuring nutritional needs are met. Now, take a deep breath, put a small portion on the tray, and enjoy the show. You’ve got this.
Sources and Further Reading:
- American Academy of Pediatrics. (2022). Amount and Schedule of Formula Feedings.
- American Academy of Pediatrics. (2022). Starting Solid Foods.
- World Health Organization. (2021). Infant and young child feeding.
- Centers for Disease Control and Prevention. (2023). How Much and How Often to Feed Infant Formula.
- Centers for Disease Control and Prevention. (2023). Foods and Drinks to Encourage.
- Mayo Clinic. (2022). Solid foods: How to get your baby started.
- Satter, E. (2000). Child of Mine: Feeding with Love and Good Sense.