
Every pregnancy journey culminates in a unique birth story. While many envision a straightforward vaginal delivery, the reality is that labor is a dynamic process, and sometimes, mother and baby need a helping hand to cross the finish line safely. This is where understanding assisted delivery methods becomes crucial. Also known as operative vaginal delivery, these procedures are not a sign of failure but rather skilled, strategic tools in an obstetrician’s repertoire. They are employed during specific challenges in the second stage of labor—when you’re fully dilated and pushing—to ensure the well-being of both you and your baby.

For expecting parents, the terms “forceps” or “vacuum” can sound daunting, often conjuring images of undue intervention. But knowledge is the antidote to fear. This comprehensive guide aims to demystify instrumental delivery, offering a clear, empathetic, and factual look at why these methods are used, how they work, and what to expect during recovery. Our goal is to empower you with information, transforming anxiety into informed confidence as you prepare for your baby’s arrival.
What Are Assisted Delivery Methods?
Assisted delivery methods, or operative vaginal deliveries, refer to the use of specialized medical instruments to help guide the baby through the birth canal during the pushing phase. The two primary instruments are obstetric forceps and the vacuum extractor. Think of them not as replacing your effort, but as augmenting it—providing gentle traction or guidance when progress stalls or when urgent delivery becomes medically necessary.
It’s important to distinguish these from a Cesarean section (C-section). An assisted vaginal birth is still a vaginal birth. The instruments facilitate the delivery through the birth canal, which can offer advantages like a quicker delivery than an emergency C-section and often a shorter recovery time for the mother. The decision to use forceps or vacuum is made in real-time by your obstetrician or midwife, based on a specific set of conditions being met and a careful assessment of what is safest in that moment.
Key Reasons for an Assisted Delivery: Understanding the “Why”
Why would your care team suggest an instrumental delivery? The reasons are always centered on the health of you and your baby. Here are the most common medical indications:
- Prolonged Second Stage of Labor: This is when pushing goes on for longer than typically expected—often more than three hours for first-time mothers (or two hours with an epidural), or more than two hours for mothers who have given birth before. Exhaustion can set in, making it harder to push effectively.
- Fetal Distress: This is a primary reason for urgent intervention. Signs on the fetal heart rate monitor may indicate the baby is not getting enough oxygen and needs to be born quickly.
- Maternal Exhaustion or Health Concerns: Conditions like severe heart disease, very high blood pressure (like preeclampsia), or extreme fatigue may mean it’s unsafe for you to continue pushing for a prolonged period.
- Certain Baby Positions: If the baby is facing upwards (occiput posterior) or is slightly angled, the doctor may use instruments to assist in gently rotating the baby to a more favorable position for delivery.
- Maternal Effort Limitations: In some cases, due to certain medical conditions or an exceptionally dense epidural block that reduces sensation, the ability to push effectively may be diminished.
The Essential Prerequisites: Safety First
Before an obstetrician can proceed with a forceps delivery or vacuum extraction delivery, several strict conditions must be met to ensure safety and maximize the chance of success:
- The Cervix Must Be Fully Dilated (10 cm): The door to the birth canal must be completely open.
- The Membranes Must Be Ruptured: The amniotic sac must be broken.
- The Baby’s Head Must Be “Engaged”: The baby’s head must have descended into the pelvis, typically at least to a zero station. The exact position of the head (like being face-down) must also be known.
- Adequate Pain Relief: This is crucial. For a forceps delivery, a robust epidural or spinal block is almost always used. For vacuum extraction, an epidural is highly recommended, though a local anesthetic can sometimes be sufficient.
- Adequate Pelvic Size: The doctor must be confident that the mother’s pelvis is large enough for the baby’s head to pass through with assistance.
- Informed Consent: Your doctor should explain the situation, the reason for the intervention, the chosen instrument, potential risks, and obtain your consent.
If these conditions are not met, a Cesarean delivery is typically the safer alternative.
A Closer Look at the Two Main Methods
Vacuum Extraction Delivery: Gentle Suction Assistance
The vacuum extractor consists of a soft or rigid cup connected to a suction pump. The cup is carefully placed on the crown of the baby’s head. Once a seal is created and gentle suction is applied, the doctor guides the traction in sync with your contractions and pushing efforts.
- Types of Cups:
- Soft Cups (Silastic or Plastic): These are more commonly used. They are pliable, may be less likely to cause scalp trauma, but can sometimes pop off (detach) if traction is too strong.
- Rigid Cups (Metal): These provide a firmer grip and are less likely to detach, but are associated with a slightly higher risk of scalp marking and bruising.
- The Step-by-Step Process:
- You are positioned, often with legs in stirrups.
- The bladder is emptied with a catheter.
- A thorough examination confirms the baby’s position.
- The chosen cup is applied to the baby’s head.
- With a contraction and your push, the doctor applies gentle, steady traction.
- Once the baby’s head crowns, the cup is removed, and the rest of the baby is delivered normally.
- Key Advantages: Generally causes less maternal perineal trauma than forceps. Often preferred when rotation of the baby’s head is not required.
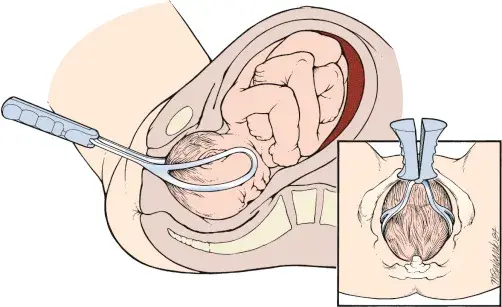
Forceps Delivery: Precision Guidance
Obstetric forceps look like two large, smooth, curved spoons or salad servers. They are designed to cradle the baby’s head, providing a firm but gentle grip. The blades are inserted one at a time and locked together. The doctor then uses them to guide or gently rotate the baby’s head and provide traction during contractions.
- Types of Forceps: Different designs serve different purposes (e.g., Simpson forceps for traction, Kielland forceps for rotation).
- The Step-by-Step Process:
- Similar positioning and preparation as for vacuum extraction.
- The obstetrician expertly slides each blade into place along the sides of the baby’s head.
- The blades are locked.
- With each contraction and push, the doctor pulls gently along the natural curve of the pelvis.
- Once the head is delivered, the forceps are removed, and the delivery is completed.
- Key Advantages: Can be more effective than vacuum for rotating a malpositioned baby. Offers a firmer grip, which can be crucial in urgent situations. May result in a slightly quicker delivery in skilled hands.
Forceps vs. Vacuum: A Side-by-Side Comparison
| Feature | Forceps Delivery | Vacuum Extraction Delivery |
|---|---|---|
| Instrument | Two curved metal blades that cradle the head. | A suction cup (soft or rigid) placed on the crown of the head. |
| Primary Use | Excellent for both traction and rotating the baby’s head. | Primarily for traction; less effective for significant rotation. |
| Maternal Trauma | Higher risk of severe perineal tears (3rd/4th degree) and episiotomy with assisted delivery. | Lower risk of severe perineal tears compared to forceps. |
| Baby’s Scalp | May cause temporary facial marking or bruising (forceps marks). | Causes a temporary swelling on the scalp called a “chignon” or cephalohematoma. |
| Success Rate | Generally has a slightly higher success rate for achieving a vaginal delivery. | Has a higher rate of “pop-off” (detachment), which may lead to a C-section. |
| Pain Relief Needed | Requires a very effective epidural or spinal block. | Can sometimes be done with a local, but an epidural is strongly preferred. |
Potential Risks and Complications: An Honest Discussion
Like any medical procedure, assisted delivery methods carry potential risks. Your doctor will only recommend them when the benefits outweigh these risks.
For the Mother:
- Increased Perineal Trauma: Higher chance of deeper tears (3rd or 4th degree) involving the anal sphincter, especially with forceps. An episiotomy is often performed to make more room and prevent uncontrolled tearing.
- Pelvic Floor Issues: Short-term or, rarely, long-term issues with urinary or fecal incontinence, or pelvic organ prolapse. [Link to article on postpartum pelvic floor exercises].
- Pain and Discomfort: Increased perineal pain, bruising, and swelling in the days following birth.
- Urinary or Bowel Issues: Temporary difficulty urinating or having a bowel movement.
- Emotional Impact: Some women may feel disappointed or traumatized by the experience, especially if it was unexpected.
For the Baby:
- Scalp Marks and Swelling: Forceps can leave temporary red marks on the cheeks; vacuum extraction causes a distinctive, round swelling (chignon) that resolves in a few days. A cephalohematoma (a collection of blood under the scalp) is also possible.
- Jaundice: The breakdown of red blood cells from bruising can slightly increase the risk of newborn jaundice.
- Retinal Hemorrhage: Small bleeds in the eyes are more common with vacuum use but almost always resolve without issue.
- Very Rare Risks: Include facial nerve injury, skull fracture, or brain bleeding, which are extremely uncommon in the hands of a skilled practitioner.
Recovery After an Assisted Vaginal Birth: Caring for Yourself
Your recovery after an assisted vaginal birth will be similar to a standard vaginal birth, but may require extra attention to perineal care.
- Pain Management: Use ice packs (for the first 24 hours), warm sitz baths, and prescribed or over-the-counter pain relievers as recommended by your doctor.
- Perineal Care: Keep the area clean and dry. Use a peri-bottle (squeeze bottle) with warm water to rinse after using the toilet. Pat dry gently; don’t wipe.
- Pelvic Floor Exercises: Begin gentle Kegel exercises as soon as you are comfortable to promote healing and restore muscle tone. [Link to article on how to perform Kegels correctly].
- Rest and Nourishment: Prioritize rest. Your body has done incredible work. Stay hydrated and eat high-fiber foods to prevent constipation, which can be painful.
- Emotional Recovery: Process your birth story. Talk about it with your partner, a doula, or a counselor if needed. It’s normal to have mixed feelings. Connecting with other mothers who had similar experiences can be very validating.
- Follow-Up: Attend your postpartum check-up. Discuss any ongoing pain, incontinence, or emotional concerns with your healthcare provider.
Can You Reduce the Chance of Needing an Assisted Delivery?
While the need for assistance often arises from unpredictable circumstances, some strategies may help promote efficient labor:
- Stay Upright and Mobile: Changing positions (walking, squatting, leaning) during labor can help the baby descend optimally.
- Consider Perineal Massage: Regularly massaging the perineum in the weeks before birth may reduce the risk of tearing and the need for an episiotomy. [Link to article on perineal massage techniques].
- Work with a Support Team: A doula or a supportive partner can provide physical and emotional comfort, which can help you manage pain and stay focused.
- Understand Your Pain Relief Options: Discuss epidural management with your anesthesiologist. A “walking epidural” or lighter dose may preserve some sensation and the urge to push.
However, it’s vital to remember: needing assistance is not your fault. It is a rational medical response to the unique challenges of your labor.
Common Concerns Addressed: Your FAQ
Is an assisted delivery considered a traumatic birth?
It can be, but it isn’t automatically so. Trauma is subjective and depends on your expectations, feelings of control, and support received. Many women feel grateful for the intervention that safely delivered their baby. If you feel distressed, your feelings are valid, and seeking support is important.
Will it affect my future ability to have a vaginal birth (VBAC)?
Not necessarily. Having a previous instrumental delivery does not preclude a future vaginal birth. The decision for a VBAC will depend on the reasons for the previous assistance and your current pregnancy.
Does it impact breastfeeding or immediate bonding?
Generally, no. Once the initial checks are done, skin-to-skin contact and breastfeeding can begin immediately, just as with an unassisted birth. Temporary bruising on the baby’s head or face does not interfere with feeding.
Conclusion: Knowledge as Your Birth Companion
Assisted delivery methods—forceps and vacuum extraction—are sophisticated, life-saving tools that have been safely used in obstetrics for generations. They represent a middle path between an unassisted vaginal birth and a Cesarean section, often allowing for a vaginal delivery when challenges arise.
The journey of birth is about safety and health, not about adhering to a rigid plan. By understanding these procedures, you move from a place of potential fear to one of partnership with your medical team. You can ask informed questions: “What are the prerequisites in my case?” “Which instrument are you considering and why?” “What are our options?”
Armed with this knowledge, you can approach your birth experience with resilience and clarity, ready to welcome your baby with confidence, no matter how they make their entrance into the world. Remember, the goal is a healthy mother and a healthy baby, and assisted vaginal birth is a valuable chapter in many beautiful birth stories.
