
Picture your six-week postpartum checkup. You are asked how you are doing, and you say “fine” — while quietly thinking about the leak when you sneezed yesterday, the heavy feeling in your pelvis when you stand too long, and a core that feels hollowed out. You are handed a quick “do your Kegels,” and you try, unsure you are even doing them right. The silent question hangs: is this just how my body is now?
Here is the clear answer: no, this is not your new normal. What you are feeling is common, but it is not inevitable. And the idea that Kegels are the single answer to postpartum pelvic floor recovery is not just incomplete — it can be counterproductive. Recovery is not about clenching in isolation; it is about re-educating a system that has been through an extraordinary event, starting with breath, awareness, and knowing when to bring in a specialist.
What the Pelvic Floor Is, and What Birth Does to It
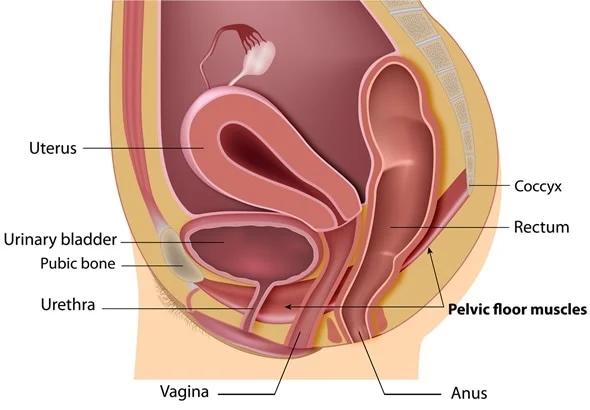
Picture your pelvic floor not as a single muscle but as a woven hammock or bowl of muscle and connective tissue, stretching from your pubic bone to your tailbone and between your sitting bones. It supports your bladder, uterus, and rectum, provides sphincter control, plays a role in sexual function, and works with your deep abdominals and diaphragm to stabilize your core and spine.
Now consider what it went through. For nine months it supported the growing weight of your baby and uterus. During birth — vaginal or surgical — those tissues were stretched, compressed, and sometimes scarred. A vaginal delivery can involve significant stretching, possible tearing, and nerve compression. A cesarean spares the pelvic floor from that descent but is major abdominal surgery that cuts through the abdominal wall and places real demand on the core to heal. The result can be weakness, tightness, or — very often — a confusing mix of both, which is exactly why a one-size-fits-all “just do Kegels” approach fails so many people.
The Key Insight: A Tight Pelvic Floor, Not Just a Weak One
Here is the shift that changes everything: many postpartum people are dealing with a pelvic floor that is too tight and non-relaxing rather than purely weak. After physical trauma — and birth is physical trauma — muscles often guard and clench to protect, which can leave the pelvic floor chronically tense (hypertonic).
A tight pelvic floor can mimic weakness: leaking with jumping, urgency, even a feeling of heaviness. But piling Kegels on top of an already-clenched muscle adds tension to tension — which can worsen pain, contribute to painful intercourse, and block true healing. That is why recovery should begin with learning to release and relax these muscles, not only contract them.
The Foundation: Diaphragmatic Breathing
Before any Kegel, start here — this is the non-negotiable foundation of postpartum core restoration:
- Lie on your back with knees bent, or prop yourself on pillows.
- Place one hand on your chest and one on your lower belly.
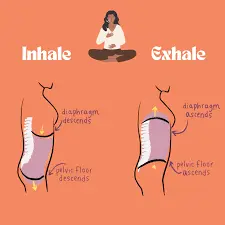
- Inhale slowly through your nose, directing the breath down into your ribs and belly so your lower hand rises. As you do, imagine your pelvic floor gently widening and descending — a soft, letting-go feeling.
- Exhale slowly through your mouth, letting your belly fall. As you exhale, think of a gentle upward lift of the pelvic floor, like a light elevator rising one floor — not a hard squeeze.
- Repeat for 5–10 breaths: inhale to expand and soften, exhale to gently engage and lift.
This re-establishes the connection you may feel you have lost (“where are they?”). It is your first and most important exercise — do it several times a day. The same breath-based technique you may have used in labor is the anchor here too.
A Progressive Exercise Guide
Phase 1 — Rest and reconnection (0–6 weeks). The goal is healing, not fitness, and always following your provider’s clearance. Continue the breathwork above, and add gentle pelvic tilts (rock your pubic bone upward on the exhale, flattening your lower back), heel slides (slide one heel along the bed and back, keeping your core stable), and short 5–10 minute walks with good posture to promote circulation. Our overview of the first six weeks postpartum sets the wider context.
Phase 2 — Rebuilding foundations (~6 weeks and up, with clearance). Now integrate gentle strength with your new connection: functional Kegels (a gentle lift on the exhale, hold 2–3 seconds, then fully release for twice as long — quality over quantity), gentle bridges (lift hips on the exhale while engaging pelvic floor and glutes), and seated marching (lift one foot an inch off the floor, alternating, keeping your core engaged).
Phase 3 — Integrating strength (~12 weeks and up, staying comfortable). Focus on coordination over isolated strength: mini-squats (hips back, exhale and engage to stand), bird-dog (extend opposite arm and leg on hands and knees, keeping the spine stable), a modified plank (hands elevated on a sturdy surface, 10–15 second holds), and standing marches. When you are ready to broaden things, our guide to returning to exercise after baby covers the next steps.
Red Flags: When to See a Pelvic Floor Physical Therapist
The guide above is a safe starting point, but the following symptoms are your body’s signal that you need a personalized assessment. Seeing a pelvic floor physical therapist is a proactive, smart step — not a last resort. Book one if you have:
- Persistent leakage: any urinary or fecal leakage beyond the first few weeks, or with coughing, sneezing, jumping, or running.
- Heaviness, pressure, or bulging: a feeling that something is falling out of your vagina, especially after standing all day — possible signs of pelvic organ prolapse.
- Pain with intercourse that persists beyond 8–12 weeks postpartum, often related to muscle tension or scarring.
- Persistent pain in your lower back, hips, tailbone, or pelvis that does not resolve with rest.
- Concerning diastasis recti: an abdominal gap that feels very deep, does not improve with gentle breathwork and pelvic tilts, or causes visible doming during activity. Our guide to diastasis recti recovery has more.
- No mind-muscle connection: a complete inability to feel or control these muscles despite focused practice.
- Pain with Kegels or bearing down, which signals dysfunction that needs assessment.
What to Expect in Pelvic Floor PT
The thought of an internal exam can feel intimidating, so here is what actually happens. A pelvic floor physical therapist treats this area with the same clinical professionalism as a knee or shoulder. A typical first visit includes a thorough interview about your birth story, symptoms, and goals; an external exam of your posture, core, hip, and spinal mobility, plus a check for diastasis recti; and — with your consent — an internal exam. That internal assessment uses a single gloved finger to check muscle tone, strength, coordination, and tenderness from the inside, which is the only way to accurately tell whether muscles are weak, tight, or uncoordinated; it should not be painful and is always explained first. From there you get a personalized plan, which may include manual therapy, biofeedback (sensors that help you “see” your muscle activity), and specific exercise progressions.
Protecting Your Pelvic Floor Day to Day
Recovery happens between exercise sessions. Protect your healing pelvic floor by lifting smart — exhale and engage your core before you lift the car seat or your toddler, holding the load close. Log-roll out of bed (roll to your side and push up with your arms rather than doing a sit-up). And manage constipation with plenty of water, fiber, and a small footstool so you are not straining.
Frequently Asked Questions
It is never too late. Pelvic floor muscles respond to training at any stage, and many people find real improvement years after their last baby. Your body can still heal and strengthen.
Yes, and it matters. Even without a vaginal delivery, pregnancy loaded the pelvic floor for nine months, and a cesarean is major abdominal surgery. The phased approach, starting with breathwork and gentle connection, is ideal — just watch your incision and avoid anything that pulls or hurts there.
This is very common, sometimes called “pelvic floor amnesia,” and it is a good reason to see a pelvic floor PT. Therapists use biofeedback and precise manual cues to help you find those muscles again, and the breathwork above is your best home starting tool.
Yes, with good form and proper core engagement. The Phase 3 mini-squat is a safe start — exhale and engage your pelvic floor and core as you stand, which supports against downward pressure. Avoid going too deep or adding weight until you have the coordination down, pain-free.
Try a gentle self-check: lie on your back with knees bent, place your fingers horizontally just above your belly button, and lift your head and shoulders slightly. Feel for the width and depth of the gap and the tension of the tissue. Improvement shows up not just as a narrower gap but as firmer tension rising under your fingers. If you see doming or “coning” during movement, step back to simpler exercises like breathwork.
The Bottom Line
Your postpartum body is not broken. Pelvic floor recovery is not about returning to a former version of yourself but about rebuilding a strong, confident foundation for the parent you are now. Listen to the signals — both the “I’m ready for a little more” ones and the clear red flags that say “I need a guide.” Seeking help is not a failure; it is advocacy for your own wellbeing. With knowledge, patience, and the right support, you can rebuild a capable core.
This article is general information, not a substitute for personalized medical advice — always work within your provider’s clearance and check with them about your own recovery.
References
- American College of Obstetricians and Gynecologists (ACOG). Exercise After Pregnancy.
- NHS. Pelvic floor exercises.
- American Physical Therapy Association (ChoosePT). Pelvic Health and Physical Therapy.
