Introduction: The Old Fear vs. The New Science
Let’s pause on a scene that plays out in countless kitchens. A parent holds a tiny spoon with a smear of peanut butter, their hand hovering near their baby’s mouth. Their heart pounds. Everything they’ve heard for decades screams, “Wait! Don’t do it! You could cause an allergy!”
I want you to take a deep breath. What you’re feeling is the echo of old, well-intentioned but fundamentally flawed advice. For years, we told parents to delay allergenic foods until ages 1, 2, or even 3. We thought we were building a fortress. In reality, we were missing a critical window—a window when a baby’s immune system is uniquely primed not for attack, but for education.

The science has undergone a seismic shift. Landmark studies, particularly the LEAP (Learning Early About Peanut) study, delivered a stunning conclusion: Early, sustained introduction of allergenic foods can dramatically reduce the risk of developing food allergies. We are not merely waiting to see if a reaction happens; we are actively training the immune system to recognize these foods as safe, nourishing friends. This is the cornerstone of the latest allergen guidelines from the American Academy of Pediatrics and global health bodies.
Your caution comes from love. But armed with new knowledge, that love can now take the form of proactive, confident action. This guide is your roadmap. We will translate complex immunology into simple kitchen steps, so you can navigate introducing allergens to babies not with trepidation, but with the quiet assurance of a parent giving their child a powerful head start toward lifelong health.
The Science in a Nutshell: Why Timing is Everything
Think of your baby’s immune system in the first year as a brilliant but impressionable student. Between 4 and 6 months of age, as the gut matures and solid foods are introduced, this system enters a critical “window of opportunity.” During this time, it is exceptionally receptive to learning what is “self” (safe) versus “non-self” (a threat).
When allergenic proteins are introduced through the gut—the intended route—the immune system is more likely to develop “oral tolerance.” It learns: This peanut protein is food, not an invader. Conversely, when the first exposure happens through inflamed, eczema-prone skin (a “leaky” barrier), the immune system can misinterpret the protein as a threat, setting the stage for an allergy. This is why early allergen introduction for eczema is not just recommended, it’s crucial.
The goal is to get the food to the immune classroom (the gut) before it gets the wrong lesson elsewhere. This isn’t a one-day field trip; it’s an ongoing curriculum. Consistency is the teacher.
The Golden Rules of Introduction: Your Foundation for Safety
Before we dive into specific foods, let’s establish the universal ground rules. These are your safety harness and success plan.
- Timing is Key: Start around 6 months of age, when your baby can sit with minimal support, shows interest in food (reaches for yours!), and has lost the tongue-thrust reflex. Do not introduce solids before 4 months.
- One at a Time: Introduce only one new major allergen every 2-3 days. This way, if a reaction occurs, you’ll know the likely culprit.
- Choose the Right Time of Day: Always offer a new allergen early in the day—ideally after a morning nap. Never offer it for the first time right before bedtime or a long car ride. You want to be alert and able to monitor for at least 2 hours.
- Commit to Consistency: A single introduction isn’t enough. Once a food is successfully introduced, you must include it in your baby’s diet regularly—aim for 2-3 times per week. This sustained exposure is what cements tolerance.
- Texture Matters: Safety first. All foods must be prepared in an age-appropriate, non-choking form. Thin, smooth, and soft are the watchwords.
Section 1: The Step-by-Step Guides – Kitchen-Tested Methods
This is your playbook. Follow these precise methods for each major allergen to maximize safety and efficacy.
Peanut
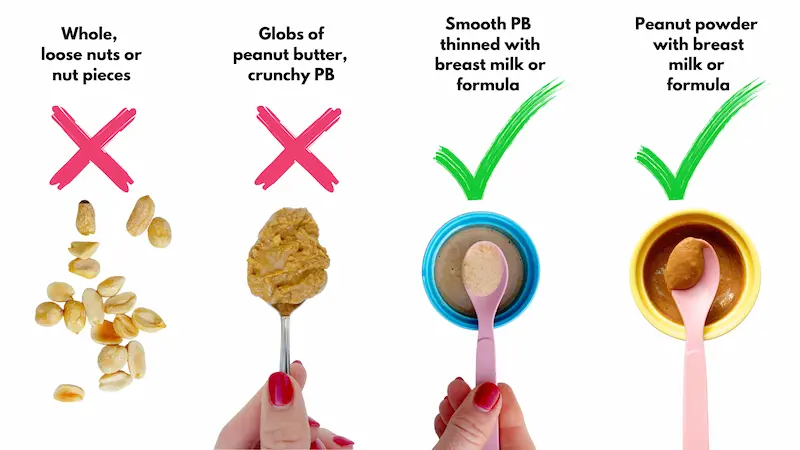
- Safe Preparation: Use smooth peanut butter. Never give whole peanuts or chunky butter. Thin 2 teaspoons of smooth peanut butter with 2-3 teaspoons of warm water, breast milk, or formula until it’s a runny, soupy paste. You can also mix a small amount of peanut powder into baby oatmeal or yogurt.
- The “First Taste” Protocol:
- Place a tiny smear (the size of a grain of rice) of the thinned mixture on your baby’s lower lip. Wait 10 minutes, watching for any immediate redness or discomfort.
- If clear, offer ¼ teaspoon of the mixture. Wait 10-15 minutes, observing closely.
- If no reaction, you can offer the remaining portion (up to 2 teaspoons total for the first session).
- What “Consistent Exposure” Looks Like: Add a dollop of thinned peanut butter to oatmeal, mix peanut powder into mashed banana, or use peanut flour in pancake batter.
Egg
- Safe Preparation: Fully cook the egg. A lightly scrambled egg with no runny yolk is perfect. Mash it finely. You can also hard-boil an egg and mash the yolk with water or avocado.
- The “First Taste” Protocol: Follow the same graduated steps: a tiny smear of cooked egg yolk or white, wait, then a small bite, wait, then a slightly larger serving.
- What “Consistent Exposure” Looks Like: Scrambled eggs, strips of omelet for baby-led weaning, egg muffins, or finely chopped egg in fried rice.
Dairy (Cow’s Milk Protein)
- Safe Preparation: Start with full-fat, plain yogurt or a small amount of finely shredded mild cheese. You can also mix a teaspoon of plain, whole-milk yogurt into a familiar puree.
- The “First Taste” Protocol: Because dairy is often less allergenic in cultured forms, you can start with a ¼ teaspoon of yogurt. Wait 10-15 minutes, then proceed.
- What “Consistent Exposure” Looks Like: Yogurt as a daily snack, cheese in scrambled eggs, cottage cheese in purees, or butter used in cooking.
Tree Nuts (Almond, Cashew, etc.)
- Safe Preparation: Use smooth, pure nut butters (e.g., almond butter, cashew butter). Thin them exactly like peanut butter to a runny consistency. Never give whole or chopped nuts.
- The “First Taste” Protocol: Use the same cautious, graduated approach as with peanut butter.
- What “Consistent Exposure” Looks Like: Alternate thinned nut butters on toast, mix nut powders into cereals, or use finely ground nut meals in baking.
Sesame
- Safe Preparation: Use tahini (sesame seed paste). Thin it significantly with water, yogurt, or a fruit puree until runny, as it can be very thick and pasty.
- The “First Taste” Protocol: Due to its potency, use an especially small starting amount (a dab on the lip) and watch closely.
- What “Consistent Exposure” Looks Like: Swirl thinned tahini into vegetable purees, use hummus (check other ingredients), or sprinkle toasted sesame seeds (finely ground) over other foods once baby is older.
Fish & Shellfish
- Safe Preparation: Cook fish (like salmon, cod) thoroughly, then flake it meticulously, checking for and removing every single bone. Mash it well. For shellfish, cook shrimp or scallops and puree or chop them incredibly finely.
- The “First Taste” Protocol: Start with a very small flake or a ¼ teaspoon of puree. Wait and observe.
- What “Consistent Exposure” Looks Like: Flaked salmon in potato mash, fish cakes, or tiny bits of shrimp in a soft pasta dish.
Section 2: Recognizing a Reaction – From Mild to Severe
This is where knowledge truly dispels fear. Knowing what to look for—and what not to worry about—is empowering.
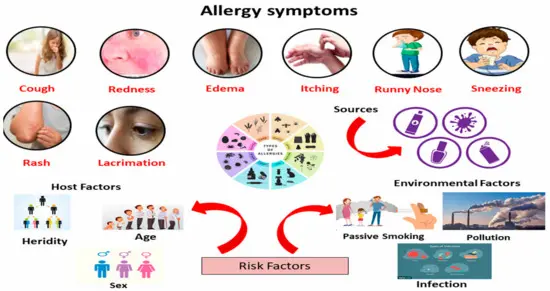
Mild/Moderate Symptoms (Monitor, Pause, Call Your Pediatrician):
- A few isolated hives around the mouth or on the body.
- Mild, transient redness or rash on the face.
- Increased gassiness or a change in stool pattern after the first introduction.
- Action: Stop feeding the new food. Monitor closely. These symptoms do not automatically mean a lifelong allergy. Contact your pediatrician for guidance on next steps, which may involve trying the food again in the office or after a pause.
Severe Symptoms – ANAPHYLAXIS (Call 911 Immediately):
- Widespread hives over much of the body.
- Swelling of the lips, tongue, or face.
- Difficulty breathing, wheezing, repetitive coughing.
- Vomiting or severe diarrhea.
- Sudden lethargy, paleness, floppiness, or collapse.
- Action: This is a medical emergency. Call 911. Tell them you suspect a severe food allergy reaction. If you have been prescribed an epinephrine auto-injector (like an EpiPen), use it immediately.
What is NOT an Allergy:
- Skin irritation from acidic foods (tomato, citrus) causing a red ring around the mouth.
- Diaper rash after eating new foods (often acidic fruits or allergens passing through).
- Gagging or spitting out due to new texture or taste.
- A single episode of spit-up. These are not immune-mediated reactions. Wiping the face quickly after acidic foods and offering textures your baby can handle will help.
Section 3: Special Scenarios & FAQs
My baby has severe eczema. What do I do?
Infants with severe eczema are at the highest risk for developing food allergies. They are the group that stands to benefit the most from early allergen introduction for eczema. The guidelines strongly recommend introducing peanut and egg as early as 4-6 months for these babies. It is often prudent to discuss this with your pediatrician first. They may recommend in-office testing (a skin prick or blood test) before a home introduction, or they may advise doing the first introduction in the office for added safety. Do not delay without medical counsel.
My baby already has a diagnosed food allergy.
This changes the plan. You must work with a pediatric allergist. Do not independently introduce other related allergens (like tree nuts if peanut allergic, or other fish if shellfish allergic) without their specific guidance, as the risk of cross-reactivity is higher.
Does what I ate during pregnancy/breastfeeding matter?
The current evidence shows that a mother’s diet during pregnancy and breastfeeding does not have a significant role in either causing or preventing food allergies in her child. Please eat a balanced, healthy diet for your own well-being. The critical factor is direct, early ingestion by the baby.
Section 4: Building a Diverse Diet – The Long Game
Think of allergen introduction not as a scary checklist, but as the exciting first chapter in raising an adventurous, healthy eater. Once you’ve successfully introduced these major foods, your job is to keep them in regular rotation. This isn’t a “one and done” vaccine; it’s more like building a muscle that needs consistent exercise.
Offer a wide variety of flavors, textures, and colors. The goal is a robust, diverse diet by age one. This ongoing exposure helps maintain the hard-won tolerance you’ve worked to establish, contributing to the broader mission of preventing food allergies in infants.
Conclusion: You Are Your Baby’s Best Advocate
You now hold the map that navigates away from fear and toward prevention. The act of offering that first tiny taste is an act of profound love and modern science. You are not playing with fire; you are lighting the way for your child’s immune system to walk a safe path.
Trust the science. Follow the steps. Watch your baby closely, but also watch with hope. You are not merely feeding your child; you are actively participating in shaping a resilient, healthy future for them—one fearless first bite at a time.
Frequently Asked Questions (FAQ)
Can I introduce allergens before 6 months?
The guidelines recommend “around 6 months.” For most babies, this is ideal. However, for high-risk infants (those with severe eczema), introduction between 4-6 months is recommended, often under medical guidance. Do not start before 4 months.
What if my baby gags or spits it out?
Gagging is a normal reflex as babies learn new textures. It is not a sign of allergy. If they spit out the taste, try mixing the allergen with a familiar, favorite food (like mixing peanut butter into breast milk or formula, then into oatmeal).
Do I need special allergen powders, or can I use regular food?
You absolutely can use regular, everyday foods! Smooth peanut butter, whole eggs, full-fat yogurt, tahini—these are perfect. Commercial mixing powders are a convenient option but are not necessary for success. The key is the protein, not the packaging.
How do I introduce shellfish safely?
Start with a well-cooked, finely minced or pureed shrimp or scallop. Mix a tiny amount into a familiar vegetable puree. Follow the standard waiting and observation protocol. Ensure there are no shell fragments.
What about sesame? It’s new on the list.
Sesame is now a major allergen. Introduction is important! Use thinned tahini as described. It’s a potent paste, so thinning is crucial to avoid a choking hazard and to allow for a very small, controlled initial dose.