
Hearing the words “incompetent cervix” or “cervical insufficiency” during pregnancy can feel like a sudden, cold shock. The language itself seems harsh, even accusatory. It’s important to begin by saying this: this diagnosis is not a reflection of your competence as a mother or a person. It is a specific, physical condition of the cervix—the structure at the bottom of your uterus that acts as a gatekeeper during pregnancy. Its job is to stay firm, long, and closed to protect your growing baby until it’s time for labor. With cervical insufficiency, that cervix begins to soften, shorten, and open painlessly and too early, often in the second trimester, raising the risk of premature birth or pregnancy loss.
This is a journey marked by profound anxiety for many women, often discovered after a heartbreaking loss. Yet, modern obstetrics offers not just understanding, but effective strategies for intervention and hope. The goal of this comprehensive guide is to demystify cervical insufficiency. We will replace fear with knowledge, explaining the causes of an incompetent cervix, the subtle symptoms of cervical insufficiency you might miss, the diagnostic process, and the proven treatments for cervical insufficiency that have helped countless women carry their pregnancies to term.
Consider this your roadmap. Whether you are researching after a loss, have been newly diagnosed, or are planning a future pregnancy with known risk factors, this information is designed to empower you to have informed, collaborative conversations with your healthcare team. Knowledge is the foundation of advocacy and, ultimately, of hope.
What Exactly is Cervical Insufficiency? Redefining the Terms
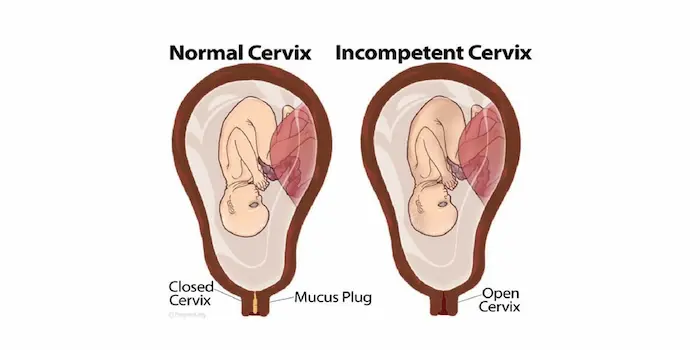
Let’s reframe the terminology first. Many medical professionals now prefer the term “cervical insufficiency” over “incompetent cervix,” as it more accurately describes a mechanical function without negative connotations. Think of your uterus as a nurturing, upside-down pear. The cervix is the narrow “stem” at the bottom. During a healthy pregnancy, this stem remains a strong, muscular sphincter—tightly closed and several centimeters long—creating a secure barrier.
In cervical insufficiency, this muscular tissue is weaker or more elastic than it should be. It cannot withstand the increasing pressure of the growing pregnancy. As the uterus expands, the insufficient cervix gradually, and usually without any pain or contractions, begins to:
- Efface: Thin out and shorten.
- Dilate: Open.
This silent, premature opening can allow the amniotic sac (the “bag of waters”) to bulge into the cervical canal, potentially rupture, and lead to preterm delivery. This often happens in the second trimester, a time when parents are just beginning to feel secure after the first-trimester milestones. Understanding this painless, progressive mechanism is key to recognizing why specific monitoring and treatments are necessary.
What Causes an Incompetent Cervix? Unpacking the Risk Factors
Unlike some pregnancy complications, cervical insufficiency often has identifiable physical causes or strong associated risk factors. It’s rarely random. Understanding these can provide crucial context, whether for diagnosing a past pregnancy or planning for a future one.
The primary causes and risk factors for cervical insufficiency fall into several categories:
- Anatomical or Congenital Factors: Some women are simply born with a cervix that has less collagen or a different muscular composition, making it inherently weaker. This can be associated with exposure to DES (diethylstilbestrol, a medication given to some women from the 1940s to 1970s) in utero.
- Traumatic or Surgical Damage (Iatrogenic Causes): This is a common cause. Any procedure that removes or damages a significant amount of cervical tissue can compromise its strength. This includes:
- LLETZ/LEEP or Cone Biopsy: Procedures used to treat cervical pre-cancer or cancer by removing a cone-shaped piece of tissue.
- Multiple Dilation & Curettage (D&C) Procedures: Especially if they involved mechanical dilation of the cervix.
- Traumatic Prior Births: A delivery that caused significant cervical lacerations.
- Pregnancy-Related Overload:
- Multiple Gestation: Carrying twins, triplets, or more places significantly more weight and pressure on the cervix.
- Polyhydramnios: An excess of amniotic fluid creates increased uterine pressure.
- Uterine Anomalies: Having a uniquely shaped uterus can sometimes distribute pressure unevenly on the cervix.
A history of second trimester miscarriage or premature birth—especially one that began with painless dilation and rupture of membranes—is the most significant clinical clue pointing toward this diagnosis. It’s often described as a loss that “came out of nowhere,” without the typical warning signs of labor.
The Silent Symptoms: What Does Cervical Insufficiency Feel Like?
This is the most challenging aspect: the changes are frequently silent. There may be no classic “labor” signs. However, some women do experience subtle cues, which are vital symptoms of cervical insufficiency to report to your doctor immediately:
- A sensation of pelvic pressure or fullness: A feeling that the baby is “pushing down” very early.
- New or increased backache: A low, dull ache that’s persistent.
- Mild abdominal cramping: Often intermittent and easy to dismiss as round ligament pain or gas.
- Change in vaginal discharge: This can be subtle. It may become more watery, mucousy, or tinged with a light pink or brown.
- A noticeable increase in vaginal discharge.
The most critical point: If you experience any of these symptoms in your second trimester—especially if you have a known risk factor—you must contact your healthcare provider without delay. Do not wait for your next scheduled appointment. Early detection is the single greatest factor in a successful intervention.
Diagnosis: How is Cervical Insufficiency Identified?
Diagnosis hinges on a combination of history and precise physical measurement. There is no single blood test. The process typically involves:
- Detailed Medical History: Your doctor will take a thorough history, focusing on past pregnancy outcomes and any cervical procedures.
- Transvaginal Ultrasound (The Gold Standard): This is the cornerstone of diagnosis and monitoring. A probe is gently placed in the vagina to obtain a crystal-clear image of the cervix. Key measurements include:
- Cervical Length: A normal cervix in mid-pregnancy is typically longer than 2.5 cm (about 1 inch). A shortening cervix, especially one measuring less than 2.5 cm before 24 weeks, is a major red flag. This is often referred to as short cervix on ultrasound.
- Funneling: This is a telling sign where the internal part of the cervix (near the baby) begins to open, creating a “funnel” or “V” shape, while the external part remains closed. It visually demonstrates the cervix giving way under pressure.
- Pelvic Exam: A physical examination can sometimes reveal a cervix that is softer than expected or beginning to dilate, but ultrasound provides far more objective and precise data.
For women with a clear history of painless second trimester dilation, the diagnosis may be made retrospectively. For those with risk factors but no prior losses, the focus shifts to preventative screening. This is why women with high-risk factors (like a prior cone biopsy or a multiple pregnancy) often have their cervical length measured serially via transvaginal ultrasound starting around 16-20 weeks.
Treatment and Intervention: The Path to a Full-Term Pregnancy
The landscape of treatment for cervical insufficiency has transformed outcomes. The approach is personalized based on your history and current ultrasound findings.
1. The Cerclage: A Stitch in Time
A cervical cerclage is the primary surgical treatment. It involves placing a strong, non-dissolvable stitch around the cervix to reinforce it, much like a purse-string, holding it closed.
- McDonald Cerclage: The most common type. It’s a simple, high stitch that can often be placed vaginally in an outpatient setting.
- Shirodkar Cerclage: A slightly more complex stitch placed slightly deeper. It may be used in specific cases or if a McDonald cerclage fails.
- Transabdominal Cerclage (TAC): A permanent stitch placed via abdominal surgery, usually around the cervix’s base. This is reserved for the most severe cases, often where a vaginal cerclage has failed or the cervix is extremely short/absent from prior surgery. It is placed before pregnancy.
Timing is crucial:
- Preventative/History-Indicated Cerclage: Placed at 12-14 weeks for women with a clear history of cervical insufficiency in a prior pregnancy.
- Ultrasound-Indicated Cerclage: Placed when serial ultrasound monitoring reveals a cervix shortening significantly (typically below 2.5 cm) before 24 weeks, even without symptoms.
- Rescue/Emergency Cerclage: A more urgent procedure attempted when the cervix has already begun to dilate and membranes are visible. This is a higher-risk intervention but can sometimes salvage a pregnancy.
The cerclage is usually removed around 36-37 weeks, allowing for a normal vaginal delivery. If labor begins before removal, the stitch must be cut immediately.
2. Progesterone Supplementation
For women with a finding of a short cervix on ultrasound but no prior history, vaginal progesterone (a hormone that helps maintain pregnancy) is a highly effective, non-surgical first-line treatment. Studies show it significantly reduces the rate of preterm birth in this group. It may also be used in conjunction with a cerclage in high-risk cases.
3. Activity Modification & Pelvic Rest
While strict, prolonged bed rest is no longer universally recommended due to risks of blood clots and muscle loss, modified activity is always advised. This means:
- Pelvic Rest: No sexual intercourse, orgasm, or placing anything in the vagina.
- Reduced Strenuous Activity: Avoiding heavy lifting, prolonged standing, and intense exercise. Listening to your body and resting when you feel increased pressure is key.
Living with the Diagnosis: Emotional and Practical Support
The emotional weight of this diagnosis is heavy. It can turn a joyful pregnancy into a time of intense vigilance and fear.
- Build Your Support Team: Lean on your partner, a trusted friend, a therapist, or support groups for women who have experienced pregnancy loss or high-risk pregnancies. You are not alone.
- Communicate with Your Provider: Ask specific questions. “What are my exact restrictions?” “What symptoms mean I should call you immediately versus going to the hospital?” Clarity reduces anxiety.
- Prepare Mentally and Logistically: With a cerclage, you will have more frequent appointments. Plan for help at home. Have a hospital bag packed earlier than usual. Knowing the plan for cerclage removal can help you visualize a positive endpoint.
- Celebrate Milestones: Each week of pregnancy gained is a victory. Celebrate making it to 24 weeks (viability), then 28, then 32. These milestones matter.
Frequently Asked Questions (FAQ)
1. Can cervical insufficiency be prevented?
Prevention focuses on managing risk. If you need a cervical procedure (like a LEEP), discuss fertility-sparing techniques with your gynecologist. Before a future pregnancy, a preconception consultation with a Maternal-Fetal Medicine (MFM) specialist is invaluable to create a monitoring and treatment plan.
2. Will I need a C-section because of this?
Not necessarily. If a cerclage is placed and later removed successfully, a vaginal delivery is often possible and encouraged. A transabdominal cerclage typically requires a C-section for delivery.
3. What are the risks of a cervical cerclage?
Risks are low but include infection, rupture of membranes, bleeding, or triggering labor/preterm contractions. The risk of not intervening when indicated is generally considered far greater.
4. If I have one successful pregnancy with a cerclage, will I need one for every pregnancy?
Yes, it is highly likely. Once diagnosed, the standard of care is to offer a preventative cerclage in subsequent pregnancies, as the underlying cervical condition remains.
5. Can lifestyle changes fix a weak cervix?
No. Cervical insufficiency is a structural issue. While avoiding heavy lifting is important, no amount of diet, exercise, or rest can fundamentally change the physical integrity of the cervical tissue. Medical intervention (cerclage, progesterone) is required.
Conclusion: From Diagnosis to Delivery – A Journey of Resilience
A diagnosis of cervical insufficiency changes the landscape of pregnancy. It introduces a vocabulary of measurement, intervention, and cautious optimism. It asks you to become an expert listener to your own body and a steadfast partner to your medical team.
But please hold onto this: this diagnosis is not an end point. It is the beginning of a specific, proactive care plan. With today’s diagnostic tools like transvaginal ultrasound and proven treatments like cerclage and progesterone, the prognosis for carrying a healthy baby to term is excellent.
Your journey may require more scans, a surgical stitch, and modified activity, but its destination remains the same: holding your newborn. Let knowledge quiet the fear. Let each step of the management plan build your confidence. You are not defined by an “incompetent” cervix, but by your incredible strength and resilience as you navigate this path to motherhood.
