That moment you peek into the crib and see a crusty, sticky eye gazing back can send a jolt of worry through any new parent. Is it an infection? Is my baby in pain? The sight of newborn eye discharge whether it’s a sleepy yellow crust, a constant watery stream, or goopy green mucus—is incredibly common and almost always looks far worse than it is. Your concern is natural, but take a breath. In the vast majority of cases, a sticky eye newborn is dealing with a simple, treatable issue.

This guide is designed to walk you through exactly what you’re seeing, why it’s happening, and what you should do. We’ll decode the symptoms, from harmless blocked tear duct baby woes to signs of infection that need a doctor’s attention. You’ll learn safe cleaning techniques, understand the “watchful waiting” approach for simple blockages, and get a crystal-clear triage list so you know precisely when to worry about baby eye goop. Consider this your roadmap from alarm to action.
What Are You Seeing? Decoding the Type of Discharge
First, don’t panic. Look closely. The color, consistency, and which eye is affected are your first clues.
- Clear & Watery: This often looks like excessive tears pooling in the eye or rolling down the cheek. It’s the hallmark of a nasolacrimal duct obstruction (blocked tear duct), where tears can’t drain normally into the nose.
- White or Cream-Colored Mucus: A stringy or sticky white discharge, often collecting in the inner corner of the eye. This is also very common with blocked ducts, as the stagnant tears become a bit mucousy.
- Yellow or Green Sticky Pus: This thicker, goopy discharge can cause the eyelids to be matted together, especially after a nap. While it can occur with a mildly irritated blocked duct, it’s also the primary sign of bacterial newborn conjunctivitis.
- Crusting That Seals the Eye Shut: Any of the above discharges can dry overnight, creating a crust that temporarily “glues” the eyelashes together. This alone is not a sign of severity.
One Eye or Both? This is a critical distinction. A blocked tear duct is almost always unilateral (affecting one eye), though it can sometimes occur in both. Conjunctivitis from an infection or irritation can easily spread to both eyes.
The Most Likely Culprit: Blocked Tear Duct (Nasolacrimal Duct Obstruction)
This is the cause of most cases of baby eye yellow crust. It’s not an infection, but a simple plumbing issue.
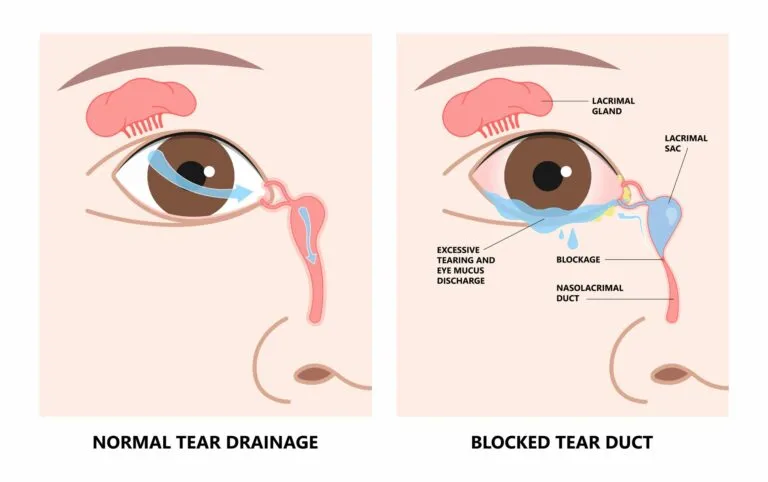
The Anatomy, Simplified: Think of the tear duct as a tiny drainage pipe. Tears are made in the lacrimal gland, wash over the eye to keep it moist and clean, and then drain through a minute opening in the inner corner of the eyelid into a tube (the nasolacrimal duct) that runs down into the nose. That’s why your nose runs when you cry. In about 20% of newborns, this drainage channel is narrow or still covered by a thin membrane at birth, causing a backup.
Hallmark Signs of a Blocked Tear Duct:
- Watery eye that always looks tear-filled.
- Mucus or mild pus in the eye, often worse after sleep.
- NO redness of the actual white part of the eyeball (the sclera).
- NO swelling of the eyelids.
- Your baby is otherwise perfectly happy, feeding well, and afebrile.
The American Academy of Pediatrics (AAP) notes that over 90% of blocked tear ducts open on their own by the time a child is one year old. Your job is to keep the area clean and perform a simple massage to encourage it to open.
When It’s More Serious: Understanding Newborn Conjunctivitis (Pink Eye)
Conjunctivitis means inflammation of the conjunctiva—the clear membrane covering the white of the eye. In newborns, it must be taken seriously and properly diagnosed. The key differentiator from a simple blockage is often redness.
Types of Newborn Conjunctivitis:
- Chemical Conjunctivitis: This is a mild irritation from the antibiotic eye ointment (usually erythromycin) given at birth to prevent serious infections. It causes mild redness and some discharge, typically appearing within the first 24-48 hours and clearing on its own within a few days.
- Bacterial Conjunctivitis:
- Common Bacterial: Caused by bacteria like staph or strep from the birth canal or environment. Symptoms include a thick, yellow-green pus, redness of the eye and inner eyelids, and swelling. It requires prescription antibiotic eye drops.
- Serious Bacterial (Ophthalmia Neonatorum): Caused by sexually transmitted infections like Gonorrhea or Chlamydia passed during birth. This is a medical emergency. The CDC emphasizes its severity: symptoms include copious pus, intense redness, and significant eyelid swelling, usually appearing 2-5 days after birth for Gonorrhea and 5-12 days for Chlamydia. It requires immediate systemic antibiotics to prevent blindness.
- Viral Conjunctivitis: Often accompanies a common cold virus. The discharge is usually more watery, and the eye is pink/red. It’s contagious but typically resolves on its own.
The “When to Worry” Triage Guide: Your Action Plan
This is the heart of the matter. Use this guide to decide your next step.
Green Zone: Likely Manageable at Home (Probable Blocked Tear Duct)
- Clear, white, or slightly yellow mucus/discharge.
- No redness in the white of the eye.
- Possible mild crusting, especially in the morning.
- Only one eye is affected (usually).
- Your baby is acting completely normal—feeding, sleeping, and alert.
Action: Proceed with gentle cleaning and tear duct massage (described below). Monitor.
Yellow Zone: Call Your Pediatrician Within 24 Hours
- Increased amount of yellow or green discharge.
- Mild pinkness or redness in the white of the eye.
- Discharge persists or worsens despite 2-3 days of proper cleaning and massage.
- You feel uncertain about the diagnosis.
Action: It’s time for a professional evaluation. Your pediatrician can confirm if it’s an infected blocked duct or conjunctivitis and prescribe antibiotic drops if needed.
Red Zone: Seek Medical Attention Immediately
- Intense Redness and noticeable swelling of the eyelids and the eyeball itself.
- Copious, thick yellow-green pus that re-accumulates quickly after cleaning.
- Your baby is under 1 month old and has any eye discharge with redness (to rule out serious infection).
- Baby shows systemic signs: fever (100.4°F/38°C or higher), extreme lethargy, refusal to feed.
- The eye appears cloudy or the cornea (clear front part) looks hazy.
- You suspect an injury or a foreign object in the eye.
Action: Do not wait. Contact your pediatrician urgently or go to an urgent care/ER. Prompt treatment for serious infections is critical.
Your Step-by-Step Home Care Toolkit
1. The Safe Cleaning Technique for Newborn Eye Discharge
This is essential for comfort and hygiene, regardless of the cause.
- Wash Your Hands thoroughly with soap and water.
- Prepare Supplies: Use sterile gauze pads or a clean, soft cotton ball for each eye. Moisten it with cooled, boiled water or sterile saline solution. Do not use tap water on its own.
- Wipe Gently: Hold the gauze/cotton ball and wipe once, softly, from the inner corner of the eye (near the nose) outward toward the ear.
- Use a Fresh Piece for Each Wipe: This is the golden rule. Discard the used piece, get a new one, moisten, and wipe again if needed. Never wipe back toward the inner corner, as this can spread debris into the duct.
- Pat Dry: Gently pat the area dry with a fresh, clean piece of gauze.

2. Blocked Tear Duct Massage (Lacrimal Sac Massage)
This gentle pressure can help open the blocked membrane. The AAP and American Academy of Ophthalmology recommend this technique.
- Wash your hands.
- Place your index finger on the side of your baby’s nose, right at the corner of the affected eye. You should feel a slight bump—this is the lacrimal sac.
- Apply firm, gentle pressure downward (toward the tip of the nose) along the side of the nose. You are not pushing on the eyeball.
- Repeat this motion 5-10 times, 2-3 times per day (ideal times: during diaper changes).
- The goal is to increase pressure in the duct to help pop open the blockage. You may see a little discharge expressed during the massage, which is fine.
3. What About Breastmilk?
A common folk remedy is to put a few drops of expressed breastmilk in the eye. While breastmilk has antimicrobial properties, there is no robust clinical evidence from sources like the AAP or CDC to support its use as an effective treatment for bacterial conjunctivitis. It is not harmful for a simple blocked duct, but it should not replace medical evaluation for a suspected infection.
Answering Your Pressing Questions
Q: How do I tell the difference between a blocked tear duct and an infection?
The single biggest sign is redness. No redness in the white of the eye = likely blocked duct. Redness + discharge = likely conjunctivitis. Also, blocked ducts are often just watery/mucousy, while infection pus is thicker and more prolific.
Q: Is it normal for the discharge to come back every morning?
Yes, absolutely. During sleep, blinking stops, allowing discharge to pool and dry. Morning crusting is typical with both blocked ducts and low-grade irritation.
Q: Will a blocked tear duct require surgery?
Rarely. If the duct hasn’t opened by 9-12 months of age, an ophthalmologist may recommend a minor probing procedure to open it. This is a quick, highly effective outpatient procedure.
Q: Could this be related to the eye ointment they got at birth?
Yes. Chemical irritation from erythromycin ointment is common, mild, and self-limiting. It should resolve within a few days.
Key Takeaways for Peace of Mind
- Don’t Panic: Newborn eye discharge is overwhelmingly common and usually benign.
- Look for Redness: It’s your primary clue for distinguishing a blocked tear duct vs eye infection.
- Clean Safely: Always wipe from the inner corner out, using a fresh wipe for each swipe.
- Massage Gently: Consistent nasolacrimal duct obstruction massage can help resolve simple blockages.
- Know the Red Flags: Fever, intense redness/swelling, copious pus, and symptoms in a baby under one month old warrant immediate medical care.
Navigating your newborn’s health is a journey of careful observation and trusting your instincts. With this knowledge, you can look at that sticky eye not with fear, but with understanding, knowing exactly how to respond to keep your little one comfortable and healthy.
References & Further Reading
- American Academy of Pediatrics (AAP). “Blocked Tear Ducts.” HealthyChildren.org. https://www.healthychildren.org/English/health-issues/conditions/eyes/Pages/Blocked-Tear-Ducts.aspx
- Centers for Disease Control and Prevention (CDC). “Conjunctivitis (Pink Eye) in Newborns.” https://www.cdc.gov/conjunctivitis/newborns.html
- Mayo Clinic. “Blocked tear duct: Symptoms & causes.” https://www.mayoclinic.org/diseases-conditions/blocked-tear-duct/symptoms-causes/syc-20351369
- American Academy of Ophthalmology (AAO). “Nasolacrimal Duct Obstruction (Blocked Tear Duct) in Children.” https://www.aao.org/eye-health/diseases/nasolacrimal-duct-obstruction-children
- National Health Service (UK – NHS). “Sticky eye in babies.” https://www.nhs.uk/conditions/sticky-eye/