
As your due date draws near, the anticipation of meeting your baby intertwines with the practicalities of birth. You might hear your doctor mention “position” and “station”—terms that describe how your baby is preparing for their grand entrance. Most babies settle head-down, but about 3-4% of full-term pregnancies find the baby in a breech position. Learning that your baby is breech can spark a wave of questions and concerns. This comprehensive guide is designed to demystify breech presentation, explain why it happens, explore your options, and ultimately empower you with knowledge and perspective for a safe and positive birth journey, regardless of the final position.
Decoding Fetal Position: From Cephalic to Breech
First, let’s visualize the landscape. In the final weeks, your baby runs out of room for grand acrobatics. They typically assume a final position, with the part of their body closest to the birth canal (the “presenting part”) leading the way.
- Cephalic or Vertex Presentation: The ideal position for vaginal birth. Baby is head-down, with their chin tucked to their chest. About 96% of babies are in this position by 37 weeks.
- Breech Presentation: Baby is positioned with their buttocks or feet down, closest to the cervix. This is the focus of our discussion.
Understanding that breech is a variation of normal fetal positioning—not a complication or something you caused—is the first step toward calm, informed decision-making.
The Three Types of Breech Presentation
Not all breech positions are the same. The specific type can influence management options and risks.
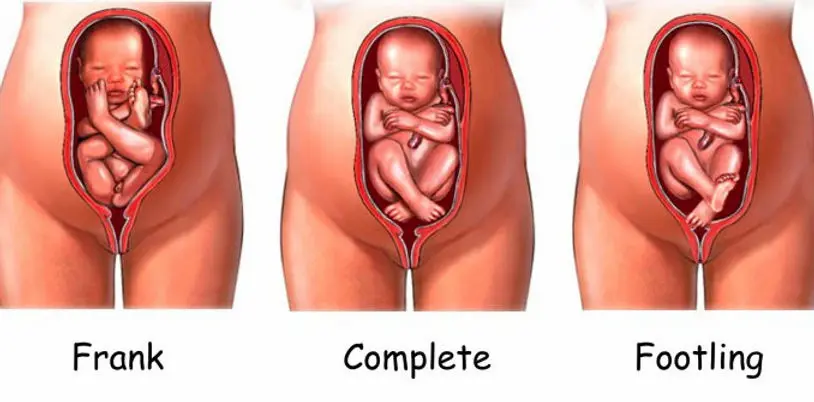
- Frank Breech (50-70% of breech cases): The most common type. Baby is in a “pike” position with their buttocks down, legs straight up in front of their body, and feet near their head. Think of a diver folded in half.
- Complete Breech: Baby sits cross-legged, with buttocks down, and knees bent with feet near the buttocks. This is like a tucked sitting position.
- Footling or Incomplete Breech: One or both feet are down, positioned to come out first. This is the least common type in full-term pregnancies.
Why Might a Baby Be Breech? Exploring the Common Causes
In most cases, there is no single, identifiable reason. It’s often a combination of factors related to the baby, the uterus, or the pregnancy itself. Think of it as your baby finding the most comfortable fit for their unique circumstances.
Common contributing factors include:
- Uterine Shape or Abnormalities: A septate or bicornuate uterus (having a divide or heart shape) can limit the baby’s room to turn.
- Placenta Location: A low-lying placenta (placenta previa) or a placenta positioned in the front (anterior placenta) can occupy the space where the head needs to go.
- Amniotic Fluid Levels: Too much fluid (polyhydramnios) gives the baby too much space to flip; too little fluid (oligohydramnios) restricts movement.
- Multiple Pregnancy: Twins or triplets have limited space, making it more common for one or more to be breech.
- Baby’s Factors: Occasionally, a congenital condition affecting muscle tone or a very large baby can make turning difficult.
- It’s Often Just Chance: For many, it’s simply the way the baby settled. It is not caused by anything you did or didn’t do.
When Breech Becomes a Focus: The Timeline of Discovery
- Before 28-32 weeks: Babies are small and float freely. A breech position at this stage is normal and not a concern. They have plenty of time to turn.
- Around 32-34 weeks: As babies get larger, they tend to settle into a position. Your provider will begin feeling (palpating) your abdomen to determine the baby’s position during prenatal visits.
- 36 weeks and beyond: This is when a persistent breech position becomes a key part of birth planning. An ultrasound will be used to confirm the type of breech, check the baby’s size, and assess amniotic fluid levels.
Your Pathway Forward: A Spectrum of Options for a Breech Baby
A breech diagnosis is not an automatic ticket to a cesarean section. It is a starting point for a conversation about risks, benefits, and choices. Your options fall into three main categories.
Option 1: Attempting to Turn the Baby – External Cephalic Version (ECV)
This is the first-line intervention for a breech baby near term.
- What it is: A procedure where an obstetrician uses their hands on the outside of your abdomen to manually encourage the baby to somersault into a head-down position.
- When: Usually performed at or after 37 weeks in a hospital setting. This timing ensures the baby is term if any complications arise.
- The Process: You’ll be monitored before, during, and after. Medication is often given to relax the uterine muscles. The doctor uses ultrasound guidance and gentle, firm pressure to lift and rotate the baby.
- Success Rate: Approximately 50-60% for first-time mothers, and slightly higher for those who have given birth before.
- Risks: Small risk of fetal distress, rupture of membranes, or placental abruption (less than 1%). This is why it’s done in a hospital with immediate access to an operating room.
- Is it painful? It can be quite uncomfortable, often described as intense pressure, but it is typically brief.
Option 2: Planned Vaginal Breech Birth
This is a highly specialized option that requires specific criteria and an experienced team.
- The Philosophy: With the right conditions and skilled practitioners, a vaginal breech delivery can be a safe alternative. Major studies (like the Term Breech Trial and its follow-ups) show that outcomes are comparable to planned C-section when strict protocols are followed.
- Key Criteria for Consideration:
- Frank or Complete Breech (not footling).
- Baby is estimated to be of normal size (not too large or too small).
- Your pelvis is deemed adequate (via clinical or imaging assessment).
- Baby’s head is in a flexed position (not extended back).
- You are in a hospital with an obstetrician, anesthesiologist, and pediatric team experienced in breech delivery.
- Labor progresses smoothly and spontaneously.
- Important Note: Many hospitals and providers no longer offer this due to a lack of training and experience following the rise of C-sections for breech. You must have a detailed, frank discussion with your provider about their experience and the hospital’s capabilities.
Option 3: Planned Cesarean Section (C-Section)
This is the most common route for breech presentation in many countries.
- Why it’s common: It eliminates the specific risks associated with a vaginal breech delivery, such as head entrapment (where the body delivers but the larger head gets stuck) or cord prolapse.
- The Procedure: A surgical delivery where the baby is born through an incision in your abdomen and uterus. For a breech baby, it is typically scheduled at 39 weeks.
- It’s a Birth, Not a Failure: Choosing or needing a cesarean for a breech baby is a valid, safe, and proactive birth choice. It is a different path to meeting your baby, not a lesser one.
Complementary & Alternative Methods to Encourage Turning
While not as evidence-based as ECV, some parents try gentle, non-invasive techniques. Always discuss these with your provider first to ensure they are safe for your specific pregnancy.
- Spinning Babies® Techniques: A set of maternal positions and movements (like the Forward-leaning Inversion) designed to create optimal space and alignment in the uterus to encourage the baby to turn.
- Acupuncture & Moxibustion: A traditional Chinese medicine technique where a practitioner burns a mugwort herb (moxa) near a specific point on the little toe. Some studies suggest it may stimulate fetal activity and increase the chances of the baby turning.
- Chiropractic Care (Webster Technique): A specific chiropractic analysis and adjustment aimed at reducing uterine constraint and balancing pelvic muscles and ligaments.
Remember, these methods work best when the baby is already active and likely to turn on their own. Their success is hard to measure but they are generally low-risk and can make you feel proactive.

Navigating Emotions and Making Your Decision
A breech diagnosis can trigger feelings of disappointment, anxiety, or a sense of lost control over your birth plan. This is completely normal.
- Grieve if you need to: If you had your heart set on a specific type of birth, allow yourself to feel that disappointment.
- Focus on Information: Shift from emotion to research. Ask your provider: “What is the protocol here? What is your experience? What are the specific risks and benefits for my situation?”
- The Ultimate Goal: A healthy parent and a healthy baby. The mode of delivery is a pathway to that goal. Empower yourself by understanding all the pathways available to you.
FAQs: Your Breech Baby Questions, Addressed
Q: Can a breech baby turn on its own at 37 or 38 weeks?
A: Yes, it is possible, but less likely as the baby gets larger and space decreases. Spontaneous turning after 37 weeks happens, but not in the majority of cases.
Q: Are there exercises I can do to help turn a breech baby?
A: The most recommended are positions that open the pelvis and use gravity. Examples include spending time on your hands and knees, pelvic tilts, and sitting forward-leaning over a birth ball. The theory is that it encourages the baby’s heavier head to swing down.
Q: Does having a breech baby mean something is wrong with my baby?
A: In the vast majority of cases, no. A breech baby is typically perfectly healthy. It is simply their position. However, in a small percentage of cases, breech can be associated with underlying conditions, which is why your provider will monitor carefully.
Q: What if my baby is breech and I go into labor before my scheduled C-section or ECV?
A: Go to the hospital immediately. Do not wait. This is a key reason for having a clear plan. The hospital team will assess you and the baby and proceed with the safest course of action, which will almost certainly be a cesarean section at that point.
Q: Will I have to have a C-section for future pregnancies if I have one for a breech baby?
A: Not necessarily. Having a prior C-section for a breech presentation is considered a “low-transverse incision,” which often makes you a good candidate for a Vaginal Birth After Cesarean (VBAC) in a future pregnancy with a head-down baby.
Q: Is an ECV worth trying?
A: For most people, yes. It’s a low-risk procedure with a significant chance of success that could allow for a vaginal birth. Even if it doesn’t work, you can move forward with your plan for a cesarean knowing you explored a good option.
Discovering your baby is breech is a twist in the birth journey, but it doesn’t have to be a crisis. It is an invitation to become an even more informed participant in your care. By understanding the types, causes, and full spectrum of options—from ECV to specialized vaginal birth to a planned cesarean—you reclaim a sense of agency. Collaborate closely with your healthcare team, ask detailed questions, and trust that whether your baby turns or not, you are moving toward a birth informed by wisdom and focused on the well-being of you both. This chapter, however unexpected, is just the prelude to the incredible story of meeting your child.
